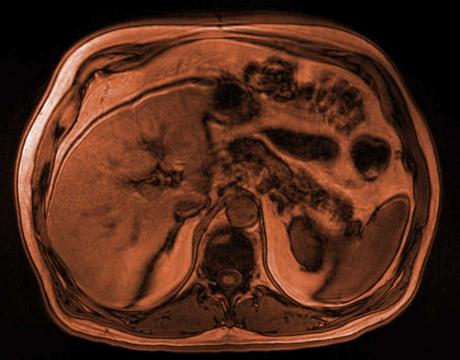
Clinical information: 77 year old male presents with central abdominal pain. Has CT abdomen and pelvis followed by an MRCP (see all images below by clicking "Study List" at the top of the PACSbin window) - what is the diagnosis?
Interesting case Abdominal 35
.png)
Salient findings:
CT:
-
Significant fat stranding and phlegmon surrounding the pancreas and the mildly oedematous pancreatic head, consistent with acute pancreatitis.
-
No abnormal enhancement of the pancreas to suggest necrosis.
-
No pancreatic duct dilation.
-
Mildly distended gallbladder but no features of acute cholecystitis.
-
No fluid collections, abscesses or pseudocysts.
-
Mild stranding through the retroperitoneum but no ascites.
MRCP:
-
No biliary duct dilation and no filling defects in the bile ducts to suggest obstructive ductal choledocholithiasis.
-
Small stones lying dependently in the gallbladder lumen (no cholecystitis).
-
The CBD can be seen draining into the main papilla of the duodenum at the Ampulla of Vater.
-
Instead of joining the CBD at the Ampulla/major papilla to drain, the main pancreatic duct of Wirsung is seen draining separately into the minor papilla, located superior to the Ampulla of Vater – features are consistent with pancreas divisum
-
The accessory pancreatic duct can be seen entering the minor papilla along with the main pancreatic duct.
-
No ventral duct is seen entering the major papilla with the CBD.
Principal Diagnosis: Acute pancreatitis with underlying Pancreas divisum (type II) anomaly
Learning points:
What is the normal embryology of the pancreatic ducts?
-
The formation of the pancreas and its ductal system occurs between the 4th and 8th weeks of gestation.
-
At 4th-5th weeks, there are two separate pancreatic buds that form:
- The ventral bud arises from the hepatic diverticulum
- The dorsal bud arises from the dorsal part of the duodenum
-
At 5-6th weeks, the duodenum rotates and in doing so, the ventral bud moves posteriorly to lie posteroinferiorly to the dorsal bud
-
At 7-8th week, the buds then fuse.
-
After fusion, the ventral bud forms the uncinate process and inferior aspect of the pancreatic head and the dorsal bud forms the superior pancreatic head, body and tail.
-
Pancreas divisum results from a failure of fusion of the ventral and dorsal bugs / anlages.
What are the types of pancreas divisum?
-
Type I (most common – 75%) : Main pancreatic duct drains vias the minor papilla and the CBD drains with the ventral duct through the ampulla of Vater
-
Type II : Same as type 1, but with absence of the ventral duct
-
Type III : Small filamentous connection between the ventral duct with the main duct prior to its drainage in to the minor papilla.
Complications:
-
Acute pancreatitis
-
Chronic pancreatitis
-
Santoriniocele
-
Diabetes
-
Chronic abdominal pain
Treatment options:
-
Usually conservative as is usually an incidental finding
-
Pancreatic enzyme supplements
-
Minor papillotomy
-
Minor papilla stenting
View our recent lectures

Latest Content
Clinical information: 77 year old male presents with central abdominal pain.
Clinical information: 36 year old male. Shortness of breath and chest pain.

Fall in shower with headache and nausea - what's the diagnosis?