Clinical information: 36 year old male. Shortness of breath and chest pain. Dyspepsia.
Interesting case Chest 14
.png)
Salient findings:
-
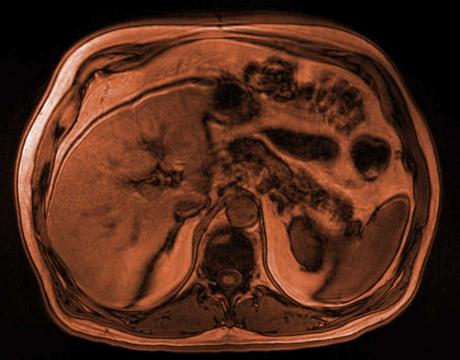
Significantly distended oesophagus which is fluid and debris filled back to its origin.
-
No gross oesophageal wall thickening.
-
No significant abnormality identified at the gastro-oesophageal junction.
-
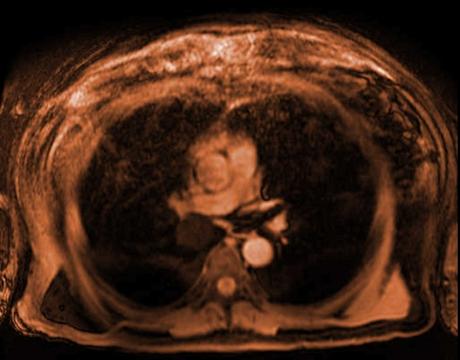
Diffuse bilateral central ground glass opacification within the lungs
-
Patchy tree-in-bud changes
-
No dense consolidation
-
Chest X ray confirms the dilated oesophagus. There is also subtle increased central hazy nodular opacification which represents the inflammation of the alveoli seen in pneumonitis.
Principle Diagnosis:
Achalasia with complication of acute aspiration pneumonitis
Learning points:
-
Achalasia v Pseudoachalasia – Primary or secondary?
-
Achalasia is a functional abnormality where the Lower Oesophageal Sphincter fails to relax due to degeneration or loss of inhibitory neurons within the myenteric plexus.
-
Pseudoachalasia results in lower oesophageal obstruction as a result of a non-functional organic aetiology.
-
-
Potential causes of Pseudoachalasia:
-
Oesophageal malignancy
-
Gastric adenocarcinoma at the gastroesophageal junction
-
Scleroderma
-
Metastatic disease to the distal oesophagus, most likely culprits being lymphoma, breast or lung ca.
-
Amyloidosis infiltration of the brainstem
-
Sarcoidosis
-
Brainstem infarcts resulting in neuropathy and denervation
-
Peptic strictures and inflammation at the cardia/GOJ
-
Post- fundoplication
-
-
How is primary achalasia diagnosed?
-
Manometry which assesses the pressure across the lower oesophageal sphincter as well as the absence of normal peristalsis
-
Secondary confirmatory tests such as barium swallow and endoscopy are often adjuncts to the investigation.
-
-
Complications of achalasia:
-
Oesophageal carcinoma
- Mid to upper oesophagus
- More likely to be a squamous cell carcinoma
- Result of food and debris stasis and resulting chronic inflammation resulting in statis oesophagitis.
-
Aspiration pneumonitis
-
Aspiration pneumonia with infection and consolidation
-
Candida oesophagitis
-
Oesophageal perforation
-
Gastroesophageal reflux disease
-
-
Usefulness of radiology?
-
Adjunctive tests such as barium swallow in the initial diagnosis
- ‘Bird’s beak’ oesophagus
-
Assessing for underlying secondary causes of Pseudoachalasia
-
Assessment of complications
-
View our recent lectures

Latest Content
Clinical information: 77 year old male presents with central abdominal pain.
Clinical information: 36 year old male. Shortness of breath and chest pain.

Fall in shower with headache and nausea - what's the diagnosis?