Clinical information: 3 days central abdominal pain and vomiting. Now, sudden hypotension and tachycardia with new pyrexia.
Interesting case Chest 13
.png)
Salient findings:
-
Hiatus hernia with oral contrast within the oesophagus, stomach and small bowel.
-
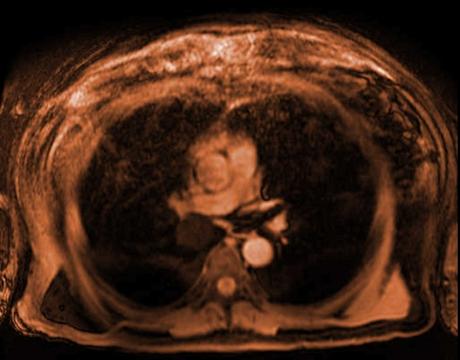
A nasogastric tube is seen traversing the lateral distal oesophageal wall and the tip lying in the left lower lobe.
-
Hyperdense collection of contrast lying in the medial aspect of the left lower lobe with multiple locules of gas measuring approximately 9.4 x 2.7 cm axially with atelectasis and hyperdense pleural effusion.
-
Features are consistent with perforation of the lower oesophagus with a nasogastric tube with a resultant collection and infective consolidation in the left lower lobe.
-
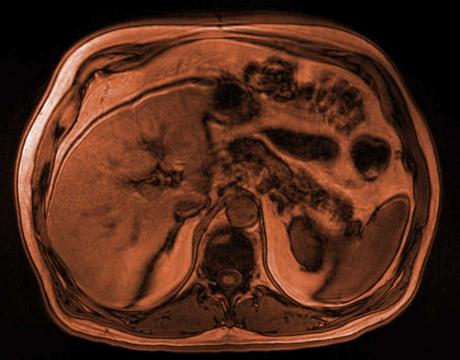
In addition, there are multiple dilated loops of small bowel throughout the abdomen and pelvis, mostly containing intraluminal contrast except for the distal most loops. There is a transition point in the medial aspect of the right iliac fossa with dilated loops extending back to the duodenum. Appearance are keeping with mechanical small bowel obstruction, possibly adhesional.
-
Quiescent pancolonic diverticular disease, more prominent in the ascending colon and caecum.
Principle Diagnosis: Perforation of the distal oesophagus/GOJ with a nasogastric tube resulting in consolidation and LRTI left lower lobe.
Other important findings: Small bowel obstruction with transition point in the right iliac fossa.
Learning points:
Causes of oesophageal perforation:
-
Traumatic insertion of nasogastric tube.
-
Long term siting of an NGT resulting in ulceration distally
-
Endoscopic procedures and stenting
-
Boerhaave’s syndrome (post vomiting spontaneous rupture)
-
Ingestion of corrosive foreign bodies resulting in oesophagitis
-
Oesophageal malignancy
Pros and cons of intraluminal small bowel contrast:
PRO: Due to better delineation of the bowel wall, lumen and adjacent structures, it can be easier to assess for strictures or areas of inflammation/wall thickening.
CON: Can reduce the conspicuity and preclude assessment of ischaemia because it can hide enhancement patterns of the bowel wall.
CON: It is often felt to be contraindicated in high grade small bowel obstruction because it can increase the likelihood of aspiration/ vomiting.
View our recent lectures

Latest Content
Clinical information: 77 year old male presents with central abdominal pain.
Clinical information: 36 year old male. Shortness of breath and chest pain.

Fall in shower with headache and nausea - what's the diagnosis?