Clinical information: Male admitted with right flank pain and haematuria ? Renal stone or hydronephrosis.
Interesting case Abdominal 34
.png)
Salient findings:
-
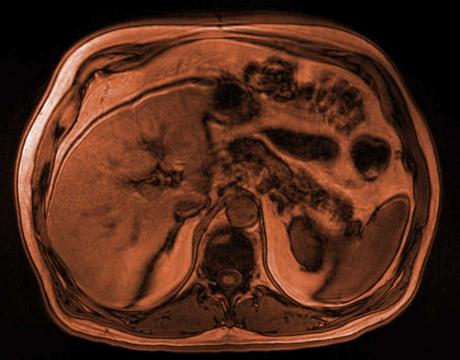
Absent left kidney with a small remnant of soft tissue in the retroperitoneum. No surgical clips in the region of the left kidney and renal vasculature to suggest previous excision.
-
Prominent contralateral right kidney measuring up to 15cm craniocaudal measured sagittally (compensatory hypertrophy) with otherwise normal appearances.
-
No right sided hydroureteronephrosis or calculi. No urinary obstruction.
-
Normal adrenal glands.
-
Fat stranding deep in the pelvis surrounding the posterior bladder, seminal vesicles and prostate.
-
Hyperdense mass-like enlargement with lobulated appearances of the left seminal vesicle which extends inferiorly to the prostate.
-
Mild oedema and swelling of the right seminal vesicle is also suggested, albeit subtle, with some adjacent stranding.
- Separate tubular structure inferolaterally indenting the bladder in the region of the left vesicoureteric junction suggestive of ureterocoele, with hypoplastic remnant of the proximal left ureter.
Principal Diagnosis:
Complications of Zinner Syndrome with vesiculitis and/or prostatitis.
Other important findings:
Ipsilateral ureterocoele
Learning points:
-
Triad of Zinner syndrome
-
-
Renal agenesis
-
Ejaculatory duct obstruction
-
Ipsilateral seminal vesicle cyst
-
-
What is the basis for Zinner syndrome embryologically?
-
Wolffian (mesonephric) duct malformation occurring at 4-13 weeks gestation
-
Early on in gestation, the ureteric bud is formed from the distal mesonephric duct which migrates cranially to induce changes in the primitive metanephric blastema of the early kidney to develop the definitive mature kidney. This occurs around 4-6 weeks of gestation.
-
Slightly later around 7 weeks, testosterone starts to influence the development of the male reproductive system as sexual differentiation begins.
-
The effect of the testosterone on the distal Wolffian duct is to form the vas deferens, the seminal vesicles and ejaculatory duct.
-
Due to abnormal development of the distal mesonephric duct between 4-13 weeks gestation, the ureteric duct either fails to form properly or fails to migrate cranially in order to form the upper renal tract. The distal duct also fails to develop adequately, resulting in atresia of the ejaculatory duct and a seminal vesicle cyst forms secondary to the accumulation and resultant backpressure of secretions.
-
Linking this back to the imaging findings in this case, you can see from the hyperdensity and enlargement of the left seminal vesicle that there is a lobulated outline of cystic spaces containing proteinaceous and sometimes haemorrhagic content, where the obstruction to the ejaculatory duct results in dilation and cyst formation and occasionally bleeding into the small cysts, explaining the appearance on CT.
-
MRI is superior to CT at anatomical delineation of location of the cysts and relationship between the cysts, the ejaculatory duct and the often ectopically inserted ureter.
-
When do patients usually present and with what symptoms?
-
Usually present in adolescence and young adulthood up to 3rd and 4th decades and often develop at the onset of sexual activity.
-
-
Clinically, patients can present with:
-
Infertility
-
Painful ejaculation
-
Recurrent prostatitis
-
Haematospermia
-
Perineal pain
-
Urinary symptoms such as dysuria and frequency
-
-
Associated findings you may see:
-
Ureterocoele on the ipsilateral side. This is a result of abnormal migration of the ureteral bud from the distal mesonephric duct resulting in ectopic insertion of the ureter, often into the ejaculatory duct or the seminal vesicle.
-
Small (or even absent) ipsilateral testis. This can also be seen depending on the point at which the gestational abnormality occurs along the process of reproductive tract development, there may be further malformations of the epididymis and/or testis.
View our recent lectures

Latest Content
Clinical information: 77 year old male presents with central abdominal pain.
Clinical information: 36 year old male. Shortness of breath and chest pain.

Fall in shower with headache and nausea - what's the diagnosis?